 by Dana Resop, MD
by Dana Resop, MD
After reviewing some ultrasound images, I recently noted that we have few archived images of procedures, although we use ultrasound in procedures often. Likely we get distracted by the procedure and forget to record screen images, but the images required vary by the procedure and this may be part of the issue.
If you have an ultrasound machine in your department, most likely this is at least partly due to the Agency for Healthcare Research and Quality (AHRQ) recommendation to use dynamic ultrasound guidance for central lines. You have devoted time and money to learn to use the ultrasound and stay proficient at it. It also costs money to keep that machine working, supply sterile probe covers and gel, as well as to support the infrastructure to get the images into the patient medical record. To reimburse you for this additional knowledge, materials and practice, there is an additional reimbursement for use of ultrasound for procedural guidance in central lines (and codes for peripheral lines, procedures, etc.)
The current CPT description for Code (76937) applies to central venous access with ultrasound guidance. The description follows.
"Ultrasound guidance for vascular access requiring ultrasound evaluation of potential access sites, documentation of selected vessel patency, concurrent real-time ultrasound visualization of vascular needle entry, with permanent recording and reporting."
Dynamic guidance recommended for vascular procedures is different from static ultrasound guidance required for paracentesis, thoracentesis or other stable, larger targets. To document static ultrasound guidance, such as for a paracentesis, ultrasound to identify the location appropriate for procedure, archive an image for the record, mark the site, then put the probe down, prep the patient and do the procedure.
In contrast, due to the dynamic nature of venous access, ultrasound is used throughout the needle placement. In a perfect world (CPT), we capture an image of the needle entering the vessel. However, attempting this may result in one of the following: broken sterile field, dropped probe, guidewire knocked off the bed, or losing the vein. Even the ACEP Ultrasound Section experts admit obtaining this image is unlikely in most ED patient settings.1
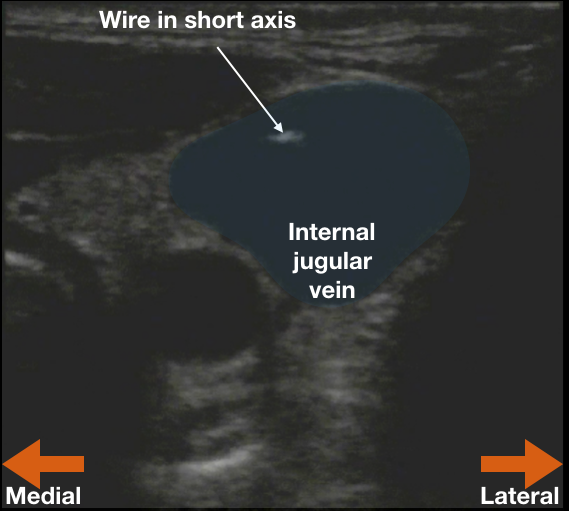
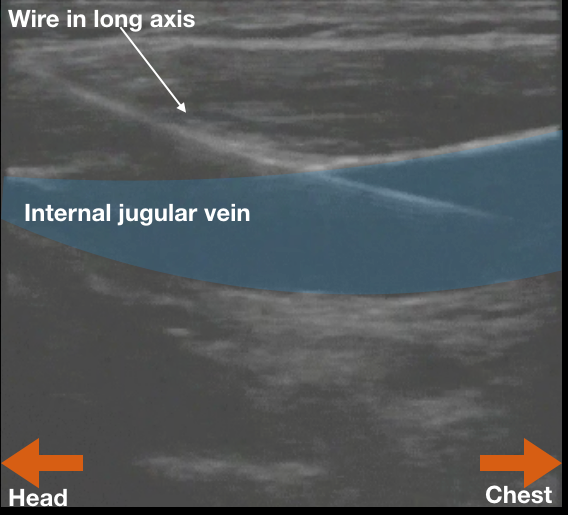 To safely document dynamic guidance during the central line procedure, use ultrasound to identify the vein, confirm patency (squish it) and then guide needle insertion. Now feed the wire into the vessel and remove the needle from the vein. Now there is nothing sharp in the patient or in the provider’s hands. Record two images of the inserted wire in the vessel: one in short-axis and one in long-axis (See figures). This is intra-procedure documentation of dynamic guidance. It also proves that the blood vessel that will shortly be dilated with a 7-French introducer (in the hypotensive patient on blood thinners) is NOT the carotid. Two wins! Remember to save the images to the patient’s chart per your department’s practice.
To safely document dynamic guidance during the central line procedure, use ultrasound to identify the vein, confirm patency (squish it) and then guide needle insertion. Now feed the wire into the vessel and remove the needle from the vein. Now there is nothing sharp in the patient or in the provider’s hands. Record two images of the inserted wire in the vessel: one in short-axis and one in long-axis (See figures). This is intra-procedure documentation of dynamic guidance. It also proves that the blood vessel that will shortly be dilated with a 7-French introducer (in the hypotensive patient on blood thinners) is NOT the carotid. Two wins! Remember to save the images to the patient’s chart per your department’s practice.
For further information about use of ultrasound, including guidelines about documenting and billing, please refer to Ultrasound the ACEP website. Experts in the ACEP Ultrasound interest group have put together multiple guidelines Multiple specialties refer to these guidelines in their own literature. I’m not a billing expert, please discuss your institution’s practice with your specialists!
1: Ref: Ultrasound FAQs (2017, Feb. 13). ACEP.org. https://www.acep.org/Physician-Resources/Practice-Resources/Administration/Financial-Issues-/-Reimbursement/Ultrasound-FAQs
Dr. Dana Resop is an EM Clinical Assistant Professor at the Univ. of WI Madison and a Board Member of WACEP. She obtained her MD at University of Wisconsin School of Medicine and Public Health, and her EM Residency and Ultrasound Fellowship training at the University of Massachusetts. She now focuses on residency education and point of care bedside ultrasound.